
With the Federal Drug Administration (FDA) on the cusp of authorizing a COVID-19 vaccine for those ages 12-15, the first group of children will become eligible in what will be an important next phase of the U.S. vaccination effort. While children are less likely to experience severe COVID-19 disease compared to adults, a small subset may develop serious illness leading to hospitalization and even death; the risk of severe disease is higher among Black and Hispanic adolescents compared to their White counterparts. In addition, since children can transmit to others, vaccinating children under age 16 will be important for achieving sufficient levels of population immunity to curb the pandemic. This is particularly the case given that the U.S. seems to have reached a COVID-19 vaccine “tipping point” among adults – that is, the point at which supply outstrips demand, making it that much harder to increase vaccine coverage. Vaccinating children may also further facilitate reopening of schools, which, in turn, will enhance the ability for parents to return to the workplace.
We examined the size and composition of adolescents ages 12 to 15 across the country using 2019 American Community Survey data to help inform vaccination efforts to reach this population. We find:
- There are almost 17 million adolescents, ages 12-15, in the United States. Adolescents account for 5.3% of the U.S. population and 26.6% of the U.S. population under the age of 16. The share of adolescents varies by state. It ranges from a low of 3.4% in DC to 6.6% in Utah.
- Nearly half of adolescents ages 12-15 are people of color, including one in four who are Hispanic, 13.4% who are Black, and 4.8% who are Asian (Figure 1). Certain states have more diverse adolescent populations. For example, over six in ten (61.4%) adolescents ages 12-15 in DC are Black, and over three in ten adolescents are Black in several other southern states, including Mississippi (41.7%), Louisiana (36.8%), Georgia (32.5%), Maryland (31.4%), and South Carolina (30.8%). States in the West and South include higher shares of Hispanic teens. For example, at least half of teens in New Mexico (62.2%), California (52.4%), and Texas (50.1%) are Hispanic.
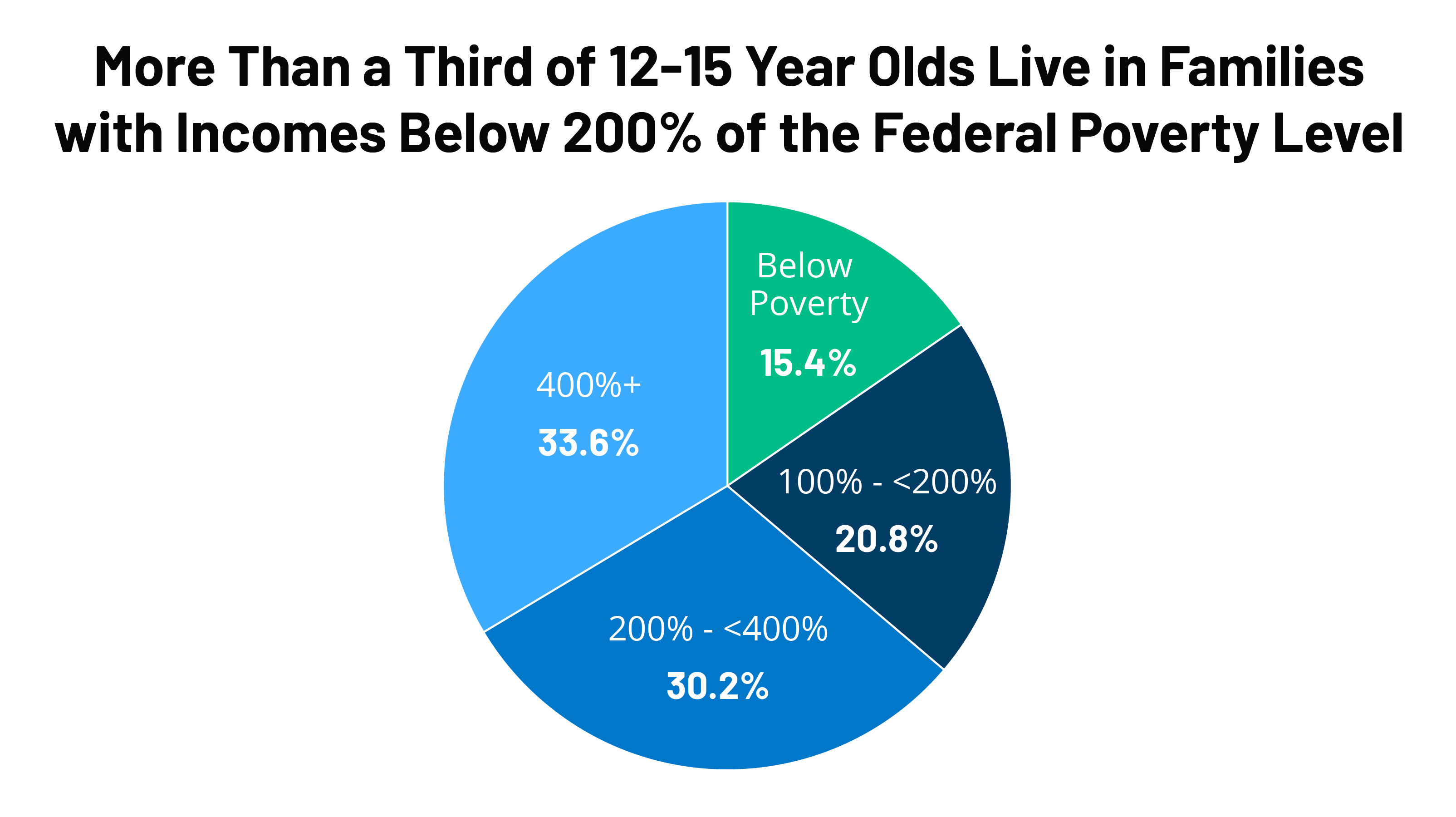
- More than a third (36.2%) of adolescents live in a family with incomes below 200% of the Federal Poverty Level (FPL), including 15.4% below poverty and 20.8% between 100-200% FPL (Figure 2). An additional 30.2% live between 200-400% FPL and 33.6% are above 400% FPL. This income distribution varies significantly by state. For example, the share of adolescents living in a low-income family (below 200% FPL) ranges from a low of 21.3% in Hawaii to a high of 49.2% in Mississippi. In 12 states, including Mississippi, the share of adolescents living below 200% FPL is greater than 40%; 10 of these states are in the South. In 5 states, more than 20% of adolescents live below the poverty level, 4 of which are in the South.
Implications
If the FDA authorizes and the Centers for Disease Control and Prevention (CDC) recommends COVID-19 vaccination for 12-15-year-olds, it will represent an important first step in reaching children more generally in the U.S. and increasing population immunity, but progress will hinge on outreach efforts and equitable and expeditious distribution strategies.
Reaching adolescents will likely take time, outreach, and effective communication to inform pediatricians, parents and adolescents about the vaccines as well as strategies to reduce barriers to access. Parents in particular will play a critical role in the success of these efforts, as our latest survey finds that 41% of parents of children ages 12-15 say they will definitely not get their children vaccinated or will only do so if required by school. These attitudes may shift once a vaccine is approved for teens and they begin receiving it, as it has for adults. Prioritizing equity and reducing access barriers that disproportionately affect people of color and those who are low income will be particularly important for reaching adolescents given the diversity of this population and that Black and Hispanic people have faced gaps in vaccinations so far.
The administration has indicated that, in addition to existing COVID-19 vaccine distribution channels, vaccines would be given directly to pediatricians to vaccinate their patients. Data from prior to the pandemic show that the large majority (96%) of children had a regular source of health care. However, analysis since the onset of the pandemic found declines in use of regular and preventive care among children, including declines in vaccination rates. This likely reflects parents delaying care due to concerns about potential exposure to coronavirus or due to cost if they experienced negative financial impacts from the pandemic. Because the vaccine is available for free regardless of insurance status, cost should not be a barrier to getting the vaccine. However, outreach to parents to explain that the vaccine is free will be important. Schools may also play an important role, including in serving as vaccine sites for children and their families.
Success in reaching this cohort will have important implications overall, for both future efforts to vaccinate those at even at younger ages and for the overall effort to vaccinate as many people in the U.S as possible.